
Last Updated on July 7, 2024 by Max
Introduction
The complexities of men’s health extend far beyond physical fitness and body composition. A crucial part of this discourse revolves around sexual health, an aspect that is often underestimated due to its sensitive nature. The most significant factors impacting sexual health are infertility, erectile dysfunction, premature ejaculation, hypogonadism, prostatitis, benign prostatic hyperplasia, prostate cancer, and an often-understated issue, testicular varicocele. Although initially causing minimal discomfort, Varicocele can serve as a breeding ground for several other sexual health problems. This blog post aims to illuminate this lesser-known but vital aspect of men’s health.
Understanding Testicular Varicocele and its Prevalence
When considering men’s health, a muscular physique or body mass isn’t the primary focus; sexual health takes precedence. Core concerns in this domain include:
- Infertility
- Erectile dysfunction
- Premature ejaculation
- Hypogonadism
- Prostatitis
- Benign prostatic hyperplasia
- Prostate cancer
- Testicular varicocele
Although testicular varicocele is often overlooked due to its relative lack of discomfort, it lays the foundation for numerous other sexual health complications. Comparable to a multi-headed beast, varicocele first hinders the normal testosterone flow from the testicles to the bloodstream, eventually impacting the testes and prostate functions throughout a man’s life. Strikingly, it is the first issue to emerge; recent studies have shown testicular varicocele prevalence in less than 1% of boys aged 2-10, yet it jumps to 15% by the time of sexual maturity (11-14 years). This suggests that venous inadequacy, specific to varicocele, primarily arises during testicular development.
Leading Causes of Testicular Varicocele
Two primary theories in the scientific literature explain varicocele occurrence:
- Anatomic differences between the left and right-side spermatic veins. The left-side vein is longer, enters the left renal vein under increased pressure, and does so perpendicularly. In contrast, the right-side internal testicular vein typically drains obliquely into the vena cava, accounting for the predominance of left-sided varicocele.
- The inadequacy of internal testicular venous valves leads to the stagnation of venous blood and increased hydrostatic pressure, which is attributed to a man’s erect posture.
Both theories partially explain the predominance of left-sided varicocele, which is ten times more common than right-sided varicocele. However, neither approach provides insight into why or how varicocele is linked to testicular development during puberty, which coincides with a peak in incidence.
A recent study by Levinger et al. found varicoceles’ prevalence is age-related. Among 504 healthy men observed, 34.7% had a varicocele. This rate increased by roughly 10% for each decade of life: 18% at age 30–39, 24% at age 40–49, 33% at age 50–59, 42% at age 60–69, 53% at age 70–79, and 75% at age 80–89.

It is posited that physical exertion during sexual maturation, but not adulthood, may lead to testicular varicocele development.
If one compares the incidence of vein varicosities in lower limbs and testicular varicocele, it becomes clear that they both stem from the exact cause. This shared cause is extreme physical tension in the organ, where vein damage is a common defensive reaction to abnormally high stress. This analogy is evident in people engaged in strenuous physical work and spending most of their day standing, leading to varicose veins. However, it could be more apparent when it comes to teenage varicocele.
The acceleration of sexual maturation in adolescents, owing to improved living conditions and increased intake of animal protein and sex hormones, leads to elevated androgen production. This surge in blood testosterone stimulates the sexual system in an immature organism and often sustains its arousal for extended periods, especially at night. This constant tension and stress in the sex organs of young people parallel the strain experienced by athletes or physical laborers.
Moreover, the changing lifestyle of the younger generation also contributes to the stagnation of venous blood in the pelvic area. The modern universal education system requires children to spend a significant amount of time sitting at school and home. While we cannot modify aspects like the erect posture of men or the anatomy of venous blood vessels, we can control what we feed our children and their education modes.
Testicular Varicocele and Male Infertility
The average rate of varicocele in the general male population is 15%, jumping to 35% in men with primary infertility and up to 80% in men with secondary infertility. Primary infertility refers to couples unable to conceive after at least one year of unprotected sex. In contrast, secondary infertility refers to couples who could conceive at least once but are now unable.
Many studies propose that varicocele or venous stasis in the internal spermatic vein increases intratesticular temperature and causes hypoxia or suffocation in the testicular tissues. This condition, in turn, deteriorates spermatogenesis and reduces testosterone production, leading to a decline in sperm quality and quantity. While most men with varicocele are fertile, the incidence of infertility among varicocele-affected men is abnormally high.

A large-scale evaluation of semen quality conducted by the World Health Organization on sperm samples from 9034 men revealed that the prevalence of varicocele in men with normal semen was more than two times lower than in men with abnormal semen quality (11.7% and 25.4%, respectively).
Moreover, a varicocele may result in testicular atrophy and dysfunctional testicular tissue. A confirmed association exists between varicocele, hypogonadism, and impaired erectile function; 30% of patients (45 out of 130) were identified with hypogonadism, while the control group reported no incidence of this condition.
Total blood testosterone is the most generally accepted indicator of hypogonadism. A study by Gorelick JI and Goldstein M revealed that varicocelectomy significantly improved serum testosterone levels in infertile men, particularly those with hypogonadism. At the same time, there are no strict lower limits for normal testosterone levels; measurements lower than 350 ng/dl should serve as a diagnostic alert for hypogonadism.
Currently, most varicocele surgeries are related to infertility issues. Approximately half of the operated men subsequently become fathers. A study by Gut Y et al. demonstrated that the treatment of testicular varicocele reinstates the flow of oxygenated blood to the testicles and revives sperm production in 4 out of 10 patients. The success rate depended on the level of irreversible damage caused by hypoxia.
Conclusion
We have explored the interrelationships between testicular varicocele, benign prostatic hyperplasia, and male infertility. It is evident that these conditions form links in a chain, and when diagnosed separately, their unity is lost, leading to an attempt to treat them as independent entities. This and future articles offer a holistic view of men’s critical sexual health issues, including varicocele, prostatitis, infertility, erectile dysfunction, premature ejaculation, and prostate cancer. A comprehensive understanding allows us to make more informed decisions and assume greater responsibility for our health. By bringing these issues into the light, we hope to inspire proactive and preventative measures in the realm of men’s sexual health. After all, the best cure is prevention, and knowledge is the first step on the path to wellness.
References
- Gat Y et al. Azoospermia and Sertoli-cell-only syndrome: Hypoxia in the sperm production site due to impairment in venous drainage of
male reproductive system. Oct 2010 · Andrologia - Gorelick JI, Goldstein M Loss of fertility in men with varicocele. Fertil Steril. 1993 Mar; 59(3):613-6.
- The influence of varicocele on parameters of fertility in a large group of men presenting to infertility clinics. World Health Organization.
- Fertil Steril. 1992 Jun; 57(6):1289-93.
Ji B , Jin XB. Varicocele is associated with hypogonadism and impaired erectile function: a prospective comparative study. Andrologia. 2017 Aug;49(6).Levinger U et al. Is varicocele prevalence increasing with age? Andrologia. 2007 Jun; 39(3):77-80.

Erectile Dysfunction & Male Sexual Vitality: How Nitric Oxide Controls Arousal, Blood Flow, and Performance
See How Nitric Oxide (NO) Changes Your 10-Year Diabetes Risk

Metabolic Health & Blood Sugar Control: The Nitric Oxide Connection

How Healthy Are Your Arteries? Take This 2-Minute Self-Check

Nitric Oxide and Endothelial Health: Protect Your Heart
Lifestyle Impact Simulator: See How Daily Habits Shape Prostate Health
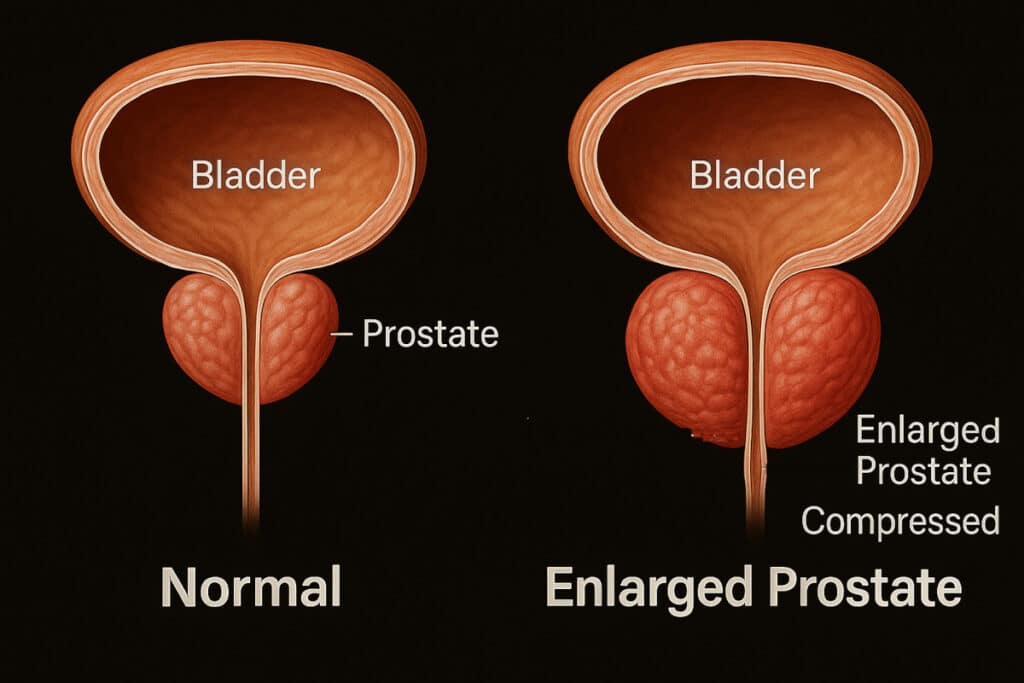
BPH Progression Slider: Visualize How an Enlarged Prostate Affects Urination
