Last Updated on August 17, 2025 by Max
Introduction
PSA is an organ-specific enzyme produced by epithelial cells of the prostate. In healthy men, most PSA is secreted into seminal fluid, liquifying semen, and only a small amount of it leaks into circulation. Normal PSA levels in the blood range between 0-2.5 ng/ml. As prostate size grows or the gland gets irritated, the blood level rises. Cancer also raises PSA because abnormal glands leak more protein into blood (National Cancer Institute, 2025).
How the PSA Test Works—And Why It Changes
PSA testing changed men’s health. Screening finds aggressive disease earlier. It also triggers anxiety and unnecessary biopsies when results reflect benign changes. The goal today is smarter PSA use—age-aware interpretation, evidence-based thresholds, and better follow-up tools (Wei, J.T., 2023).
The lab reports PSA in ng/mL. Total PSA includes protein that binds to blood proteins plus a “free” fraction. Free PSA clears fast—about two hours—while complexed PSA lingers for two to three days; that difference explains short-term bumps after irritation and the slower fall after treatment (Richardson, T.D., 1996; Brändle, E., 1999).
Several everyday factors raise PSA for a short period. Ejaculation and vigorous cycling increase PSA for up to 48 hours; a recent biopsy, infection, or prostatitis can keep levels up for weeks. Plan testing after these issues settle, and avoid ejaculation and hard cycling for two days beforehand (National Cancer Institute, 2025; Tchetgen, M.B., 1996).
Certain medications lower PSA. Finasteride and dutasteride cut PSA by about 50% after six to twelve months. Clinicians interpret results by doubling the measured value in men on these drugs (Salisbury, B.H., 2024; FDA, 2018).
Based on age, what PSA level might trigger visiting a urologist?
- 40–49 years: up to 2.5 ng/mL
- 50–59 years: up to 3.5 ng/mL
- 60–69 years: up to 4.5 ng/mL
- 70–79 years: up to 6.5 ng/mL
These thresholds come from large population-based studies and are consistent with American Urological Association (AUA) and NCCN guidelines (Oesterling, J.E., 1993; Carter, H.B., 2013).
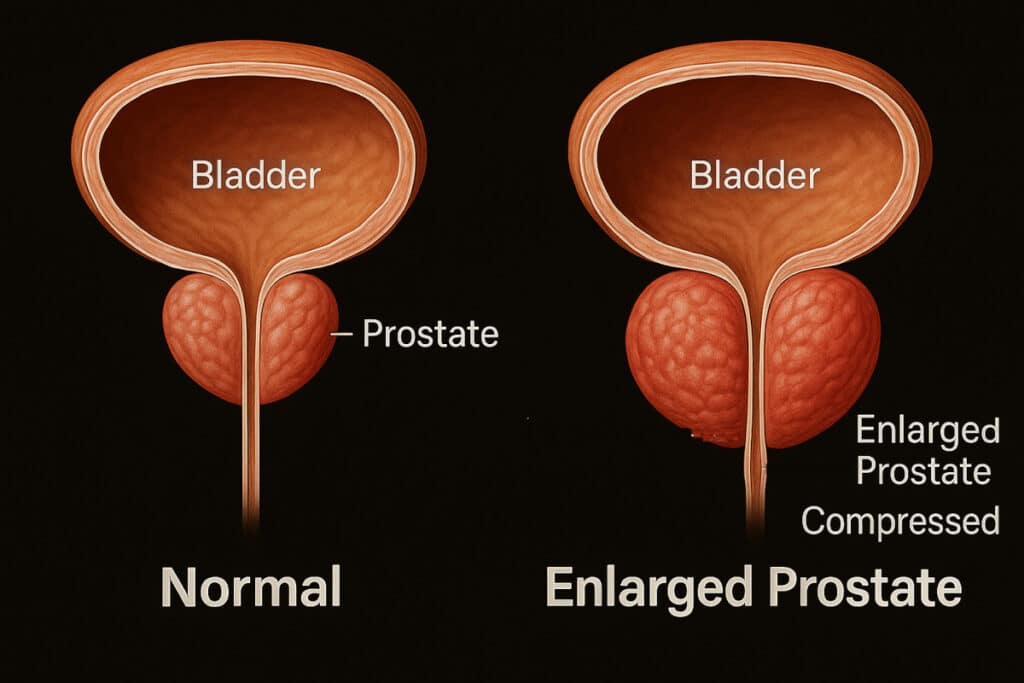
So the architecture of the prostate tissue keeps PSA confined to the gland. However, any disease condition of the prostate, whether it’s cancer, inflammation (prostatitis), or benign prostatic hyperplasia (BPH), may compromise the integrity of the prostate tissue and increase the level of PSA leaked into circulation and detected by the PSA test. Moreover, prostate massage, biopsy, or transurethral resection of the prostate can also elevate the serum PSA level. So, none of the PSA triggering factors boost the real PSA synthesis in the prostate cells; PSA expression in cancer cells was found to be even slightly depressed. Moreover, the incidence of prostate cancer in men with PSA levels below the accepted level of 4.0 ng/mL was found to be comparable to that of patients with PSA between 4.0-10.0 ng/mL. All the said allow stating that PSA should not be used as a prostate cancer marker.
What Big Trials Say About Screening
The European Randomized Study of Screening for Prostate Cancer (ERSPC) shows a clear mortality benefit with time. After 16 years, PSA-based screening reduced prostate cancer deaths; the benefit grew with repeat testing (Hugosson, J., 2019). Follow-ups continue to show fewer advanced cancers and disease progression with organized screening programs (Hogenhout, R., 2024).
U.S. guidance emphasizes shared decisions. The AUA/SUO recommends offering screening from 45–50 for average-risk men, earlier for high-risk groups, and discourages routine screening in men with limited life expectancy (Wei, J.T., 2023). The USPSTF advises individual decisions for ages 55–69 and against routine screening at 70+ (U.S. Preventive Services Task Force, 2018).
Smarter Triage After an Elevated PSA
1) Repeat the test under clean conditions. Confirm a new elevation after at least two days without ejaculation or hard cycling, and once any urinary infection or prostatitis resolves. Many “spikes” settle on retest (National Cancer Institute, 2025).
2) Use reflex tools that improve specificity. When a man’s total PSA result falls into the “gray zone” of 4–10 ng/mL, the challenge begins. PSA can rise for many reasons, not just prostate cancer — benign prostatic hyperplasia (BPH), prostatitis, and even recent ejaculation may push the number up. That’s where reflex tests step in to sharpen the picture.
Percent free PSA
One of the most widely used reflex tools is percent free PSA. Here’s how it works. PSA exists in the blood in two major forms:
- Bound PSA – attached to proteins in the blood.
- Free PSA – circulating unbound.
Prostate cancer tends to release more bound PSA, while benign conditions release proportionally more free PSA. So, by calculating the ratio of free PSA to total PSA (called “percent free PSA”), doctors get a more specific signal of whether the elevation is suspicious.
Why It Matters in the 4–10 ng/mL Range. The gray zone is tricky: only about 25% of men with PSA between 4–10 ng/mL actually have cancer on biopsy (Catalona, W.J., 1998). That means 3 out of 4 men may undergo unnecessary biopsies if PSA alone drives the decision.
This is where percent free PSA saves the day:
- If percent free PSA is ≤25% → the risk of cancer rises significantly. Doctors usually recommend biopsy in this case.
- If percent free PSA is >25% → the risk drops. Many of these elevations turn out to be benign, so a biopsy may be safely avoided.
For example, in a man with PSA = 6 ng/mL:
- Free PSA = 0.9 ng/mL → percent free PSA = 15%. This strongly suggests higher risk of prostate cancer.
- Free PSA = 2.0 ng/mL → percent free PSA = 33%. This points more toward a benign condition like BPH.
Using this ratio does two critical things: 1. Improves specificity – it filters out benign cases, so doctors don’t over-diagnose. 2. Reduces unnecessary biopsies – sparing men from discomfort, anxiety, and possible complications.
That’s why most modern guidelines recommend percent free PSA as a reflex test before sending men with PSA 4–10 ng/mL straight to biopsy.
Prostate Health Index (PHI)
The Prostate Health Index (PHI) blends total PSA, free PSA, and p2PSA – a PSA subform more strongly linked with prostate cancer.. It outperforms PSA alone and trims avoidable biopsies, especially in the 2–10 range (Lee, I-T., 2025; Leung, J.S.L., 2023).
PHI = (p2PSA / free PSA) × √(total PSA).
This formula may sound technical, but the principle is simple: PHI adds an extra cancer-linked signal (p2PSA) to refine accuracy. Higher PHI values = higher probability of significant prostate cancer. A PHI score above 40 is strongly associated with clinically relevant cancer, helping physicians decide when a biopsy is essential (Loeb, S., 2015).
PHI has shown superior performance compared to free PSA alone in predicting aggressive cancers, which means fewer men undergo unnecessary biopsies while still catching the dangerous cases.
4Kscore
The 4Kscore test takes reflex testing even further. It measures four blood-based kallikrein markers:
- Total PSA
- Free PSA
- Intact PSA
- Human kallikrein 2 (hK2)
These markers are fed into an algorithm that also factors in age, digital rectal exam (DRE) results, and prior biopsy history. The output? A personalized risk percentage of finding high-grade (Gleason ≥7) prostate cancer if a biopsy were done (Vickers, A.J., 2010).
The beauty of the 4Kscore is its focus on clinically significant cancer. It helps doctors avoid chasing indolent, harmless cancers while making sure aggressive ones don’t slip through.
All three reflex tools — percent free PSA, PHI, and 4Kscore — share the same mission: Together, they transform PSA from a blunt instrument into a precision tool for modern prostate cancer detection.
3) Bring MRI into the pathway. Modern programs use PSA to trigger multiparametric MRI. Men with PSA ≥3 ng/mL often proceed to MRI first. Lesions rated PI-RADS 4–5 go to targeted biopsy; men with PI-RADS 1–3 get risk-based management that includes PSA density (often ≥0.15–0.20) (Uroweb/EAU, 2024; Pellegrino, F., 2022). Trials such as STHLM3-MRI confirm that biomarker-plus-MRI strategies detect significant cancer while limiting unnecessary biopsy (Nordström, T., 2024).
What Your Number Means Today
Context drives meaning. A PSA of 3.2 in a 52-year-old sits close to the age-typical ceiling, but the story changes if last year’s value was 1.1, if cycling happened the day before, or if prostatitis flared last month. A PSA of 4.8 in a 68-year-old may be “typical” by decades-old population data yet still deserves a careful modern work-up, especially if density runs high or MRI shows a lesion (Oesterling, J.E., 1993; Wei, J.T., 2023).
Practical Prep Before Testing. Schedule the blood draw when you feel well. Skip ejaculation and hard cycling for 48 hours. Delay testing six to eight weeks after prostatitis, a urinary infection, instrumentation, or a biopsy. Tell your clinician if you take a 5-alpha-reductase inhibitor so results get interpreted correctly (National Cancer Institute, 2025; Salisbury, B.H., 2024; FDA, 2018).
Conclusions
Summing up all of the above, one can conclude:
- PSA may be used as a sign of prostate tissue integrity.
- Leakage of excess PSA into the bloodstream may be caused by various factors, including prostate cancer.
- Do your PSA test only to know the health status of your prostate, without any reference to prostate cancer.
In my opinion, it was a great mistake to approve the use of the PSA test to screen asymptomatic men for prostate cancer. We know that a high rate of PSA may indicate the presence of a prostate tumor. But it is the same as we know that people who have more than 100 birthmarks are more prone to skin cancer. It is good to be aware of that to take care of skin health and avoid harmful contacts that may trigger malignant transformation. However, this is not a cause of constant concern, affecting the quality of life and forcing long visits to doctors.
Do your PSA test to assess the health status of your prostate.
References
- Catalona, W.J., 1998. Use of the percentage of free PSA to enhance cancer detection and reduce unnecessary biopsies. JAMA. PubMedJAMA Network
- FDA, 2018. Drug Safety Communication: 5-alpha reductase inhibitors reduce PSA ~50% by 6 months; interpret results accordingly. FDA.gov. U.S. Food and Drug Administration
- Hogenhout, R., 2024. From screening to mortality reduction: ERSPC 21-year perspective. Eur Urol Oncol. euoncology.europeanurology.com
- Hugosson, J., 2019. A 16-year follow-up of ERSPC shows screening lowers mortality with repeated rounds. Eur Urol. PMCEuropean Urology
- Lee, I-T., 2025. Clinical utility of the Prostate Health Index (PHI). The Prostate. PubMedWiley Online Library
- Leung, J.S.L., 2023. PHI triage reduces unnecessary biopsies with low miss rate for significant cancer. Diagnostics. PMC
- National Cancer Institute, 2025. PSA Fact Sheet: factors that transiently raise PSA; patient prep. cancer.gov. Cancer.gov+1
- Nordström, T., 2024. Secondary analysis of STHLM3-MRI: biomarker-plus-MRI improves screening yield. JAMA Netw Open. JAMA Network
- Oesterling, J.E., 1993. Age-specific reference ranges for PSA in healthy men. JAMA. PubMed
- Pellegrino, F., 2022. PSA density cutoffs in the MRI era: ≥0.20 preferred over 0.15. Eur Urol Focus. PMC
- Richardson, T.D., 1996. Free PSA half-life ≈110 minutes vs 2–3 days for total PSA. Urology. ScienceDirect
- Salisbury, B.H., 2024. 5-alpha-reductase inhibitors halve PSA; double values for interpretation. StatPearls. NCBI
- Tchetgen, M.B., 1996. Ejaculation raises PSA for up to 48 hours. Urology. PubMed
- Uroweb/EAU, 2024. Diagnostic evaluation chapter: MRI-first pathways and PSA density use. EAU Guidelines. uroweb.org
- U.S. Preventive Services Task Force, 2018. PSA screening recommendation: shared decisions age 55–69; against routine screening at 70+. USPSTF. USPSTF+1
- Wang, J.C., 2024. 4Kscore alongside MRI improves prediction of Grade Group ≥2 cancer and guides biopsy. JU Open Plus. Lippincott Journals
- Scuderi, S., 2023. U.S. trends and evidence: 4Kscore reduces biopsy rates in practice. Eur Urol Open Sci. eu-openscience.europeanurology.com

Prostate Problems in Dogs: What Dog Owners Need to Know

Mastering the Moment: Your Guide to Overcoming Premature Ejaculation
BPH Progression Slider: Visualize How an Enlarged Prostate Affects Urination

Lifestyle to Mitigate Prostatitis Symptoms

Prostate Cancer: Looking For the Roots

Prostate cancer screening and early detection do NOT save men’s lives. Let’s do the math. Per the USPSTF (U.S. Preventive Services Task Force): “Only one man in 1,000 could possibly have a life-saving benefit from screening” and “A small benefit and known harms from prostate cancer screening”. However about 1.3 to 3.5 deaths per 1,000 from prostate blind biopsies. Also, 5 men in 1000 died and 20.4% had one or more complications within 30 days of a prostatectomy. This does not include deaths, injuries, and side effects from radiation and other procedures, medical mistakes, increased suicide rate, ADT therapy complications, heart attacks, depression, low quality of life, etc, caused by prostate cancer screening and treatments. Detection and overtreatment for prostate cancer have killed or destroyed millions of men’s lives worldwide from understated and multiple undisclosed side effects. The doctor that invented the PSA test, Dr. Richard Ablin now calls it: “The Great Prostate Mistake”, “Hoax” and “A Profit-Driven Public Health Disaster”. Follow the money!
<-- My story: http://www.yananow.org/display_story.php?id=1659 https://www.youtube.com/watch?v=tYii98gcejA https://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/prostate-cancer-screening1 https://medium.com/@drsadeghi/early-detection-disaster-4d4740ee5828 https://urologyweb.com/ https://urologyweb.com/uro-health-blog/ https://grossovertreatment.com https://medium.com/@bvorstman/is-psa-testing-for-prostate-cancer-bad-health-advice-7199618e56c5 https://www.youtube.com/watch?v=0IHE9jdCpn4 --/>
Recommended books:
The Great Prostate Hoax by Richard Ablin MD (the inventor of the PSA test)
The Big Scare, The Business of Prostate Cancer by Anthony Horan MD.
Hi JJ
Thanks for stopping at my blog and commenting. It is difficult to disagree with the opinion of a person who has received the best service of modern medicine. And you can’t argue against the facts. It’s no secret that human health is the most convertible business. As I noted in the conclusion of the post “it was a great mistake to approve the use of the PSA test to screen asymptomatic men for prostate cancer”.
I wish you health and long life!
Makhsud