
Last Updated on September 28, 2025 by Max
Introduction
An erection is a vascular performance. Nitric oxide (NO) acts as the biochemical key that unlocks penile blood vessels and launches the cascade that fills the penis with blood (Burnett, A.L., 2007). Nerve endings and the lining of blood vessels unleash NO the moment arousal begins. This tiny gas flips a molecular switch that relaxes smooth muscle and allows rapid, powerful blood flow (Burnett, A.L., 2007). Erectile dysfunction touches men of all ages, yet its odds climb with time. Clinical reviews place ED rates in single digits under age 50 and above 30% by the sixth decade (Leslie, S.W., 2024). Importantly, ED often signals broader vascular trouble. Large pooled analyses show men with ED face roughly a 40% higher risk of future cardiovascular events (Dong, J.Y., 2011). In short, sexual function reveals heart health.
In this post, you will learn how NO drives arousal and blood flow, why NO declines, practical steps to restore NO, and how drugs fit into the biology. You will get clear, evidence-based actions you can start this week.
- Introduction
- How an erection works — the nitric oxide signal
- How Nitric Oxide Drives Arousal and Erection
- Why Nitric Oxide Fails — Common Causes of Impaired NO Signaling and ED
- How Nitric Oxide Actually Drives Arousal, Blood Flow, and Performance
- Clinical assessment — when to act, what tests to run, and why timing matters
- Protecting and restoring the NO pathway — practical, science-first strategies
- Pharmacologic & procedural therapies — what works, when to use it, and what to expect
- Conclusion
How an erection works — the nitric oxide signal
An erection is a fast, mechanical event powered by chemistry. Nerve endings in the penis and the vascular lining release nitric oxide (NO) the instant arousal begins. This tiny gas slips across cell membranes and flips a single molecular switch: soluble guanylyl cyclase (sGC). sGC then pumps up cyclic GMP (cGMP) inside smooth-muscle cells. Rising cGMP relaxes the smooth muscle, widens penile arteries, and floods the corpora cavernosa with blood. The result is a rapid, pressurized engorgement that becomes—and stays—an erection. (Burnett, A.L., 2007).
Two enzymes make most of the NO the penis needs. Neuronal NO synthase (nNOS) provides the burst from nerve endings during sexual stimulation. Endothelial NOS (eNOS) supplies a steadier NO tone from the blood-vessel wall. Together they create a precise on/off signal that times blood flow to sexual activity. (Toda, N., 2005).
Medical therapy exploits this chemistry. Phosphodiesterase type-5 (PDE5) breaks down cGMP and ends the erection. PDE5 inhibitors block that breakdown, so cGMP stays high longer and erections strengthen. These drugs work for a large majority of men with vascular ED, and their mechanism confirms NO’s central role. (Andersson, K.E., 2018).
Biology gives us useful numbers, not just metaphors. In a placebo-controlled trial, oral L-citrulline raised penile NO availability and improved erection hardness from mild ED to normal in 50% of participants versus 8% on placebo. That result shows small metabolic changes can produce clinically meaningful gains. (Cormio, L., 2011). Meanwhile, animal and human physiology studies show that blocking NO synthase abolishes erections entirely—direct proof that NO is the physiological effector of erection. (Burnett, A.L., 1992).
Why NO fails in many men. Chronic disease and aging blunt NO production and signaling. Endothelial dysfunction, insulin resistance, and smoking lower eNOS activity. Neuropathy and pelvic nerve injury reduce nNOS signaling. Low NO equals lower cGMP, narrower arteries, and faster PDE5-driven shutdowns. Clinically, that translates into slower engorgement and incomplete erections. (Burnett, A.L., 1997; Toda, N., 2005).
Practical takeaway: support the NO pathway to protect sexual function. Lifestyle moves that improve endothelial health—regular aerobic exercise, smoking cessation, glucose control, and treatment of high blood pressure—preserve NO production and preserve erections. When necessary, targeted therapies (PDE5 inhibitors, arginine/citrulline supplementation, or future sGC modulators) restore the chemical cascade rather than masking symptoms. (Andersson, K.E., 2018; Menafra, D., 2022).
How Nitric Oxide Drives Arousal and Erection
Nitric oxide (NO) is the biochemical spark that starts sexual arousal’s hydraulic engine. Nerves and the endothelium release tiny bursts of NO during sexual stimulation. NO diffuses into nearby smooth-muscle cells and flips a molecular switch. (Montorsi, P., 2005). At the molecular level, NO binds and activates soluble guanylate cyclase (sGC). sGC converts GTP into cGMP, the second messenger that relaxes smooth muscle. cGMP activates protein kinase G (PKG), lowers intracellular calcium, and relaxes the cavernosal smooth muscle. The result: arterial inflow rises, venous outflow compresses, and the corpora cavernosa trap blood — penile rigidity follows as intracavernosal pressure rises toward systemic levels. The enzyme PDE5 trims cGMP back down. When PDE5 activity dominates, cGMP falls fast and the erection ends. That is exactly the target of modern oral drugs: PDE5 inhibitors preserve cGMP levels, prolong relaxation, and restore functional blood flow.
Importantly, erectile dysfunction often signals vascular trouble earlier than heart disease. Multiple clinical studies show ED commonly appears 2–5 years before a first cardiovascular event. Men with ED have an elevated cardiovascular risk; a large meta-analysis reported about a 48% higher risk of future cardiovascular disease versus men without ED. Younger men show an even stronger predictive signal. (Montorsi, P., 2005) (Hodges, L.D., 2007) (Dong, J.Y., 2011) (Vlachopoulos, C., 2013)
Practical takeaway: supporting endothelial health preserves NO signaling. Lifestyle steps that improve endothelial function — exercise, smoking cessation, healthy weight, and glucose control — protect the NO → sGC → cGMP pathway and thus sexual function.
Why Nitric Oxide Fails — Common Causes of Impaired NO Signaling and ED
Nitric oxide is fragile. It’s produced in bursts, diffuses quickly, and is vulnerable to biochemical sabotage. When NO availability falls, the whole cascade — sGC activation, cGMP production, smooth-muscle relaxation — falters. The result is poor blood inflow and failed rigidity. Endothelial dysfunction is the central villain. In many chronic diseases, endothelial nitric-oxide synthase (eNOS) becomes “uncoupled.” Instead of making NO, it generates superoxide and other reactive oxygen species. That both lowers NO bioavailability and increases oxidative stress — a double hit that weakens vasodilation across the body, including the penis. (Cyr, A.R., 2020)
Diabetes is among the strongest clinical risk factors. Across pooled studies, about half of men with diabetes show erectile dysfunction; type-2 disease and older age push prevalence higher. Hyperglycemia drives advanced glycation, endothelial damage, and impaired NO signaling. (Kouidrat, Y., 2017)
Tobacco smoke and nicotine directly damage NO pathways. Smoke reduces both neuronal and endothelial NOS activity and floods tissues with superoxide. Long-term smokers show significantly higher ED rates and slower recovery of vascular function after quitting. (Tostes, R.C., 2008)
Hypertension, high cholesterol, obesity, and metabolic syndrome all share one common endpoint: reduced NO signaling because of inflammation and oxidative stress. Each condition chips away at endothelial health, so ED appears as an early, visible symptom of systemic vascular disease. (Vlachopoulos, C., 2013)
At the molecular level, other biochemical culprits exist. Elevated asymmetric dimethylarginine (ADMA) blocks NOS. Chronic inflammation raises cytokines that blunt NO responses. Together these factors lower the NO pulse size and shorten its lifetime in tissue. (Dong, J.Y., 2011)
Clinical signal and implications. ED frequently appears before heart disease. The “artery size” idea explains this: smaller penile arteries block earlier than larger coronary vessels, so impotence often precedes angina or an MI by 2–5 years. Men with ED have an elevated cardiovascular risk; a large meta-analysis reported roughly a 48% higher risk of future cardiovascular disease. Younger men show an even stronger predictive signal. (Montorsi, P., 2005) (Hodges, L.D., 2007) (Dong, J.Y., 2011) (Vlachopoulos, C., 2013)
Practical, evidence-based takeaways: restore NO by treating the cause. Tight glucose control, smoking cessation, blood-pressure management, lipid lowering, weight loss, and exercise reduce oxidative stress and restore endothelial function. Where indicated, PDE5 inhibitors preserve cGMP levels and can bridge function while longer-term vascular repair proceeds. (Montorsi, P., 2005) (Dong, J.Y., 2011)
How Nitric Oxide Actually Drives Arousal, Blood Flow, and Performance
Nitric oxide is the spark that flips the switch on penile blood flow. First, nerves and endothelial cells release NO in short, targeted bursts during sexual arousal. NO diffuses across tiny gaps and finds an enzyme called soluble guanylate cyclase (sGC). sGC instantly converts GTP into cyclic GMP (cGMP). cGMP acts as a second messenger that activates protein kinase G (PKG). PKG lowers intracellular calcium and relaxes the smooth muscle surrounding penile blood channels. Relaxed smooth muscle lets arterial inflow surge and venous outflow compress, trapping blood and producing rigidity. This cascade happens fast — seconds to minutes — which explains why NO is so tightly tied to moment-to-moment sexual function. (Moncada, S., 1991) (Ignarro, L.J., 1998)
The intracellular cGMP pool is the key amplifier. Higher cGMP equals stronger relaxation and larger penile cross-section. The enzyme phosphodiesterase type 5 (PDE5) breaks cGMP down rapidly. When PDE5 activity rises, cGMP falls and the erection weakens. PDE5 inhibitors block that breakdown, preserving cGMP and prolonging smooth-muscle relaxation — the pharmacologic logic behind sildenafil and its class. (Goldstein, I., 1998)
Importantly, NO production itself depends on healthy endothelium and neuronal NOS isoforms (eNOS and nNOS). Oxidative stress, glycation, and inflammation shrink the NO pulse and shorten its reach. That’s why systemic vascular disease shows up as sexual dysfunction first in many men. Younger men with ED often have a clearer vascular signal because they lack competing age-related causes. (Montorsi, P., 2005) (Vlachopoulos, C., 2013)
Quantitative cues you can use clinically and practically: reduced NO bioavailability and lower cGMP link to measurable declines in penile blood flow and Doppler metrics. Meta-analyses report higher future cardiovascular risk in men with ED, and PDE5 inhibitors raise cGMP enough to restore flows measurable by duplex ultrasound in many cases. Those data anchor NO’s central role in both physiology and therapy. (Dong, J.Y., 2011)
Takeaway in one line: NO is the immediate messenger that opens the blood gates; cGMP is the volume control; PDE5 is the off-switch — protect the first two, and the last one becomes less relevant. (Moncada, S., 1991) (Ignarro, L.J., 1998) (Goldstein, I., 1998)
Clinical assessment — when to act, what tests to run, and why timing matters
Treat erectile dysfunction as more than a bedroom problem. Early-onset ED often signals failing blood vessels elsewhere. Men with new ED have higher short- and long-term cardiovascular risk. (Dong, J.Y., 2011)
First step: take a focused history. Ask about onset, severity, morning erections, libido, medications, and lifestyle. Screen for chest pain, exercise tolerance, and unexplained fatigue. Then measure blood pressure, BMI, and waist circumference. A structured history finds red flags fast.
Second step: basic, high-yield labs. Order fasting glucose or HbA1c, a lipid panel, and a morning total testosterone when clinical signs suggest low androgens. These tests spot common, reversible causes that damage NO signaling. (AUA Guideline, 2018)
Third step: cardiovascular triage. Use a structured risk approach. Men with ED and active cardiac symptoms need prompt cardiology evaluation. Men with ED without symptoms deserve systematic risk-factor assessment and optimization. The Princeton recommendations advise evaluating cardiovascular risk in men with ED as standard care. (Princeton III, 2012)
Why urgency matters. The “artery-size” idea explains timing: small penile arteries fail earlier than large coronary vessels. Thus ED can precede angina or myocardial infarction by 2–5 years, creating a prevention window. Act now, and you can reduce later heart attacks. (Montorsi, P., 2005)
How to use diagnostic imaging selectively. Reserve penile Doppler ultrasound for men with ambiguous histories or suspected vascular lesions after initial workup. Use cardiovascular stress testing when the risk classification demands it. Follow guideline-based, stepwise decision rules. (AUA Guideline, 2018)
Put it together: triage + treat. Optimize glucose, lipids, blood pressure, weight, and smoking status. When appropriate, start PDE5 inhibitors as first-line pharmacotherapy while addressing vascular health in parallel. Longitudinal data show ED identifies men at higher future cardiac risk, especially younger men, so early intervention matters. (Vlachopoulos, C., 2013)
Protecting and restoring the NO pathway — practical, science-first strategies
Nitric oxide is fragile. Fight the forces that snuff it out, and sexual function often follows. Start with lifestyle. Move daily. Aim for a mix of aerobic and resistance training — both improve endothelial function and boost NO bioavailability. Regular exercise raises flow-mediated dilation (a standard endothelial test) and repairs the vascular signals that feed sGC. (Green, D.J., 2018). PMC
Eat like your vessels matter. A Mediterranean-style pattern — lots of olive oil, vegetables, nuts, and oily fish — lowers cardiovascular events and preserves endothelial health. That diet nurtures NO by cutting inflammation and oxidative stress. (Estruch, R., 2013). New England Journal of Medicine
Quit smoking and control glucose. Smoking generates reactive oxygen species that grab NO and neutralize it. Poor glycemic control glycate eNOS and shortens NO’s reach. Tight glycemic control, smoking cessation, and weight loss restore NO pulses and shrink vascular risk. (Montorsi, P., 2005). PubMed
Treat the numbers that damage NO. Statins, ACE inhibitors/ARBs, and modern diabetes drugs improve endothelial function beyond their primary targets. Use them when risk-factor optimization requires medication. These agents restore the biochemical soil where eNOS and nNOS operate.
Use PDE5 inhibitors correctly. PDE5 drugs block cGMP breakdown. That raises intracellular cGMP and amplifies the NO signal, improving penile blood flow and sexual performance. Large randomized trials demonstrated consistent benefit versus placebo. (Goldstein, I., 1998). New England Journal of Medicine
Consider targeted adjuncts when appropriate. High-quality trials and meta-analyses show oral L-arginine (and arginine-rich combinations) improves erectile metrics in men with mild–moderate ED, often at daily doses in the 1,500–5,000 mg range in trial protocols. Use supplements as adjuncts, not replacements for proven therapies. Monitor interactions and side effects. (Rhim, H.C., 2019). PubMed
For refractory vascular ED, advanced options exist. Low-intensity shockwave therapy, intracavernosal injections, and vascular surgery are specialist paths. Choose these after careful vascular testing. Always align interventions with cardiovascular risk management.
Practical care pathway (concise)
- Step 1 — confirm history and screen for red flags.
- Step 2 — optimize lifestyle: smoking stop, Mediterranean diet, structured exercise.
- Step 3 — treat risk numbers: glucose, lipids, blood pressure.
- Step 4 — start PDE5 inhibitor when appropriate and review response.
- Step 5 — refer to urology/cardiology for persistent vascular ED or abnormal testing.
Numbers to remember: men with ED show higher future CVD risk (meta-analysis RR ≈ 1.48). Use that window to prevent heart attacks by aggressive risk management now. (Dong, J.Y., 2011).
Pharmacologic & procedural therapies — what works, when to use it, and what to expect
Treatments sit on a simple principle: raise cGMP, widen the corpora, and preserve blood in the penis.
Start with the least invasive, scale up when needed, and always screen for cardiac contraindications first.
Oral PDE5 inhibitors are first-line. They help most men and restore potency quickly for many. Large meta-analyses show clear superiority versus placebo, with network estimates that commonly place overall benefit in the ~60–80% range depending on population and drug. (Madeira, C.R., 2021). PDE5 drugs are generally safe when used correctly, but they interact dangerously with nitrates. Screen medications and cardiac status before prescribing. (Kloner, R.A., 2004).
When PDE5 inhibitors fail or are unsuitable, intracavernosal injections remain highly effective. Classic large studies report that men can achieve functional sexual activity with injections in the majority of attempts — efficacy in trials often exceeds 70–90% per injection session. These injections demand training and follow-up, but they work when oral therapy does not. (Linet, O.I., 1996). New England Journal of Medicine+1
Low-intensity shockwave therapy (LiSWT) is a noninvasive option that aims to restore tissue perfusion and endothelial function. Meta-analyses and randomized trials report modest, sustained improvements in erectile scores for many men, especially those with mild-to-moderate vascular ED. Protocols still vary, so set expectations accordingly. (Yao, H., 2022).
Treatment chooser — simulate expected effects
Combination and salvage strategies fill gaps. Combining oral agents with lifestyle change, intracavernosal therapy, or targeted interventions increases success for many. Injectable prostaglandins and combination injection mixes retain strong efficacy, though adherence can fall due to injection anxiety and inconvenience. (Duncan, C., 2019). PubMed
Practical caveats for clinicians and patients
- Always screen for nitrates, unstable angina, or recent myocardial infarction before starting PDE5 inhibitors. (Kloner, R.A., 2004).
- Set realistic expectations: oral drugs work well for most, but about 20–40% need alternative strategies. (Madeira, C.R., 2021).
- Teach safe injection technique and rotate sites. Monitor for fibrosis, priapism risk, and patient comfort. (Linet, O.I., 1996).
- Use LiSWT selectively: it helps some patients, particularly those with vascular ED, but protocols and effect sizes vary. Discuss uncertainty. (Yao, H., 2022).
Conclusion
Nitric oxide is the engine that drives normal erection. When endothelial cells and nerves release NO, sGC activates and cGMP rises. Smooth muscle relaxes, vessels widen, and blood fills the corpus cavernosum. This biochemical cascade anchors sexual performance and links erectile function tightly to vascular health (Burnett, A.L., 2007). PMC
Clinically, erectile dysfunction often arrives before heart disease. ED commonly precedes a first cardiovascular event by roughly 2–5 years. Therefore ED is not only a quality-of-life problem; it functions as an early vascular alarm. Use an ED complaint to trigger cardiovascular risk assessment. (Montorsi, P., 2005) (Hodges, L.D., 2007).
For therapy, two themes run through the evidence. First, restore NO/cGMP signaling to restore function. PDE5 inhibitors block cGMP breakdown and improve erections acutely, but they do not directly repair damaged microvessels. Second, regenerative approaches such as low-intensity shockwave therapy aim to repair the endothelial network. Trials and reviews show promising signals for LiSWT, especially in men with vascular ED; benefits develop over weeks and often persist longer than drug effects. Still, trial protocols vary, and results remain heterogeneous. (Dong, J.Y., 2011) (Vardi, Y., 2010) (Lu, Z., 2017) (Yuan, F., 2021).
Safety matters. Never combine nitrates with PDE5 inhibitors. Ask patients about nitrate use before any pharmacologic step. For device-based therapies, use validated clinical systems and trained operators. Home gadgets do not reproduce clinical dosing and carry safety and efficacy risks. (FDA labels; clinical reviews).
Put it together in practice: treat symptoms, treat risk. Improve lifestyle, optimize cardiovascular risk factors, and restore NO signaling pharmacologically or with targeted therapies when appropriate. When ED appears, use it as a prompt for a cardiovascular workup, not only for a prescription. (Montorsi, P., 2015)
References
- Montorsi, P., 2005) Montorsi P. The artery size hypothesis: a macrovascular link between erectile dysfunction and coronary artery disease. Am J Cardiol. 2005.
- Hodges, L.D., 2007) Hodges LD. The temporal relationship between erectile dysfunction and cardiovascular disease. Int J Clin Pract. 2007.
- Dong, J.Y., 2011) Dong JY, et al. Erectile dysfunction and risk of cardiovascular disease: a meta-analysis of prospective cohort studies. J Am Coll Cardiol. 2011.
- Vlachopoulos, C., 2013) Vlachopoulos C., et al. Erectile dysfunction and cardiovascular risk: a systematic review and meta-analysis of cohort studies. Eur Heart J. 2013.
- Burnett, A.L., 2007) Burnett AL. The role of nitric oxide in erectile function. J Sex Med (review). 2007.
- Toda, N., 2005) Toda N., et al. Nitric oxide and penile erectile function. (physiology review). 2005.
- Bivalacqua, T.J., 2006) Bivalacqua TJ., et al. Endothelial nitric oxide synthase keeps erection. (mechanistic review). 2006.
- Vardi, Y., 2010) Vardi Y., et al. Can low-intensity extracorporeal shockwave therapy improve erectile function? A 6-month pilot study. Eur Urol. 2010.
- Vardi, Y., 2012) Vardi Y., et al. Clinical and physiological effects of LI-ESWT on ED in PDE5i responders. J Urol. 2012.
- Lu, Z., 2017) Lu Z., et al. Low-intensity extracorporeal shockwave treatment for erectile dysfunction: review and meta-analysis. J Sex Med. 2017.
- Yuan, F., 2021) Yuan F., et al. Low-intensity extracorporeal shockwave therapy for ED: umbrella review of systematic reviews and meta-analyses. World J Mens Health. 2021.
- Gruenwald, I., 2013) Gruenwald I., et al. Shockwave treatment of erectile dysfunction. Andrologia / review. 2013.
- Bocchino, A.C., 2023) Bocchino AC., et al. Systematic review: LI-ESWT clinical efficacy for erectile dysfunction. 2023.
- StatPearls, Dhaliwal A., 2023) Dhaliwal A., PDE5 inhibitors: mechanisms, interactions, and contraindications. StatPearls. 2023.
- FDA / DailyMed labels) Prescription drug labeling for PDE5 inhibitors: contraindication with organic nitrates. See sildenafil/tadalafil/vardenafil labels (DailyMed / FDA).
- Montorsi, P., 2015) Montorsi P., et al. ED: exception or early marker? Follow-up and clinical implications. 2015. d
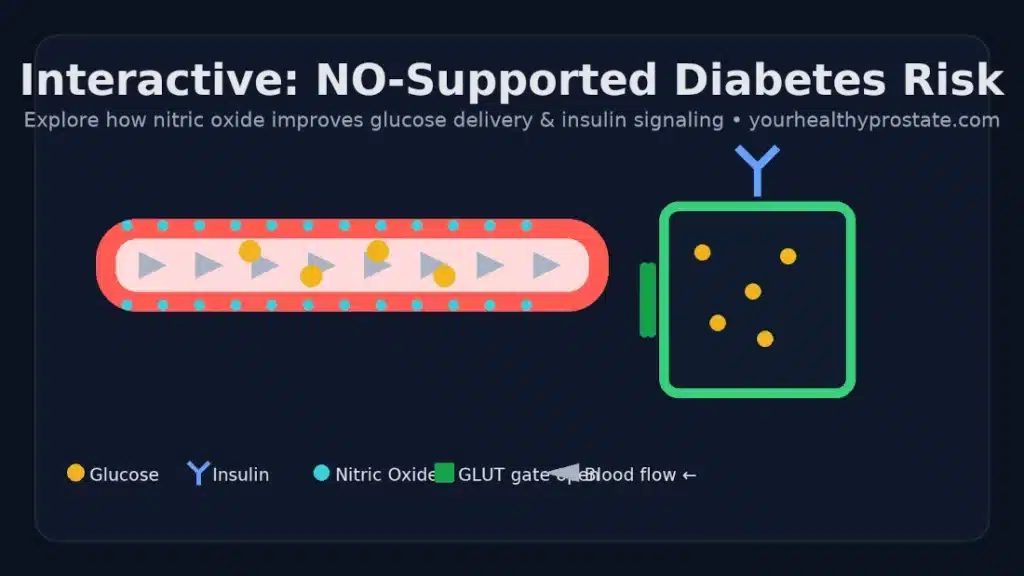
See How Nitric Oxide (NO) Changes Your 10-Year Diabetes Risk
Decoding Prostate Cancer Risk: Understanding the Factors and Steps to Mitigation

A Message From a Man Diagnosed With Prostate Cancer

Managing Prostatitis at Home – A Personal Experience
High-Fructose Corn Syrup (HFCS): A Sweetener with a Bitter Aftertaste
